Celecoxib, marketed as Celebrex, belongs to a class of nonsteroidal anti-inflammatory drugs (NSAIDs) known as COX-2 inhibitors. These drugs were developed to alleviate pain and inflammation, particularly in conditions like arthritis, with the promise of being gentler on the stomach compared to traditional NSAIDs. However, concerns have emerged regarding their cardiovascular safety, leading to restrictions and heightened scrutiny around their use. This article delves into the reasons behind these restrictions, exploring the evidence that has prompted health agencies to issue warnings and guidelines concerning celecoxib.
Cardiovascular Risks Associated with Celecoxib: The Evidence
The initial appeal of COX-2 inhibitors was their selective action, targeting cyclooxygenase-2 (COX-2) enzymes, which are primarily involved in inflammation and pain. Traditional NSAIDs inhibit both COX-1 and COX-2, with COX-1 playing a role in protecting the stomach lining. However, clinical trials began to reveal a concerning trend.
One of the pivotal studies that raised alarms was the Adenomatous Polyp Prevention on Vioxx (APPROVe) trial, which led to the withdrawal of rofecoxib (Vioxx), another COX-2 inhibitor, from the market in 2004 due to increased cardiovascular risks. Following this, the focus shifted to celecoxib. The Adenoma Prevention with Celecoxib (APC) study investigated the use of celecoxib for preventing colorectal adenomas. This study inadvertently provided crucial data on cardiovascular safety.
In the APC trial, over 2000 patients were randomized to receive either placebo or celecoxib at doses of 200 mg twice daily or 400 mg twice daily. After approximately three years, researchers observed a dose-related increase in cardiovascular events, defined as death from cardiovascular causes, myocardial infarction (heart attack), stroke, or heart failure. The results were striking:
- Placebo group: 1% experienced cardiovascular events.
- Celecoxib 200 mg twice daily group: 2.3% experienced cardiovascular events (hazard ratio [HR] 2.3).
- Celecoxib 400 mg twice daily group: 3.4% experienced cardiovascular events (HR 3.4).
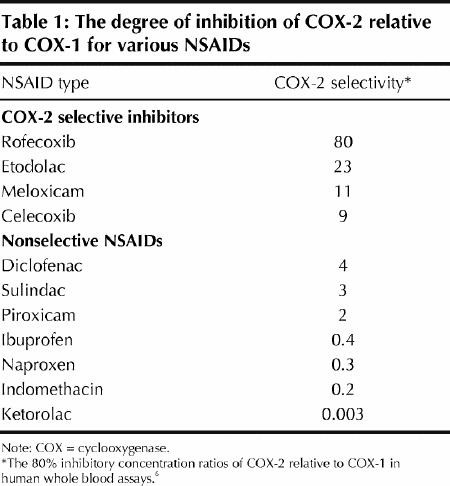 COX-2 Selectivity of Common NSAIDs: A Table Comparing Relative COX-2/COX-1 Ratios for Pain Management
COX-2 Selectivity of Common NSAIDs: A Table Comparing Relative COX-2/COX-1 Ratios for Pain Management
These findings indicated a clear association between celecoxib use and an elevated risk of cardiovascular events, and importantly, this risk appeared to increase with higher doses.
Broader Context: Valdecoxib and NSAID Safety
Concerns about cardiovascular risks weren’t limited to celecoxib. Valdecoxib (Bextra), another COX-2 inhibitor, also faced scrutiny. A study involving patients undergoing coronary artery bypass grafting (CABG) found a higher incidence of cardiovascular events in those receiving valdecoxib and parecoxib (another COX-2 inhibitor) for post-operative pain management compared to placebo. Valdecoxib was eventually withdrawn from the market due to these cardiovascular safety concerns as well as reports of severe skin reactions.
These events prompted a broader re-evaluation of the safety profile of all NSAIDs, both selective and non-selective. Regulatory bodies like the US Food and Drug Administration (FDA) and Health Canada took action, mandating that all prescription and over-the-counter NSAIDs include warnings about potential cardiovascular, gastrointestinal, and other risks.
Recommendations for Celecoxib Use and Risk Mitigation
In light of the evidence, health authorities have issued recommendations to guide the use of celecoxib and minimize potential cardiovascular risks. Key guidelines include:
- Risk Assessment: Healthcare providers are advised to assess a patient’s baseline cardiovascular risk before prescribing celecoxib. Tools like Framingham risk calculators can be used for this purpose.
- Contraindications: Celecoxib is generally not recommended for patients with pre-existing cardiovascular disease, diabetes, or other significant cardiovascular risk factors.
- Lowest Effective Dose and Shortest Duration: When celecoxib is deemed necessary, it should be prescribed at the lowest effective dose for the shortest duration possible to manage symptoms. Long-term use requires careful consideration of the risk-benefit profile.
- Alternative Pain Management: Exploring alternative pharmacologic and non-pharmacologic pain management strategies is strongly encouraged, especially for patients at higher cardiovascular risk. It is important to note that aspirin (ASA) is unique among NSAIDs as it is known to reduce both primary and secondary cardiovascular events. The cardiovascular risk associated with other non-selective NSAIDs remains less clear but is still a consideration.
Conclusion: Balancing Benefits and Risks
While celecoxib can be an effective option for managing pain and inflammation, particularly for individuals who are at high risk of gastrointestinal side effects from traditional NSAIDs, its use is not without risks. The evidence clearly indicates an increased risk of cardiovascular events, especially with higher doses and prolonged use. Consequently, celecoxib is not “banned” outright, but its use is restricted and requires careful patient selection, thorough risk assessment, and consideration of alternative treatments. Patients and healthcare providers must engage in informed discussions about the potential benefits and risks to make the most appropriate treatment decisions, prioritizing patient safety and well-being.
